Over active bladder
Overactive bladder syndrome is common. Symptoms include an urgent feeling to go to the toilet, going to the toilet frequently, and sometimes leaking urine before you can get to the toilet (urge incontinence). Treatment with bladder training often cures the problem. Sometimes medication may be advised in addition to bladder training to relax the bladder.
Understanding urine and the bladder
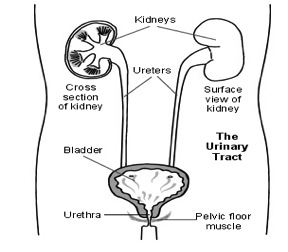
The kidneys make urine all the time. A trickle of urine is constantly passing to the bladder down the ureters (the tubes from the kidneys to the bladder). You make different amounts of urine depending on how much you drink, eat and sweat.
The bladder is made of muscle and stores the urine. It expands like a balloon as it fills with urine. The outlet for urine (the urethra) is normally kept closed. This is helped by the muscles beneath the bladder that sweep around the urethra (the pelvic floor muscles).
When a certain amount of urine is in the bladder, you become aware that the bladder is getting full. When you go to the toilet to pass urine, the bladder muscle contracts (squeezes), and the urethra and pelvic floor muscles relax.
Complex nerve messages are sent between the brain, the bladder, and the pelvic floor muscles. These tell you how full your bladder is, and tell the right muscles to contract or relax at the right time.
What is overactive bladder syndrome?
An overactive bladder is when the bladder contracts suddenly without you having control, and when the bladder is not full. Overactive bladder syndrome is a common condition where no cause can be found for the repeated and uncontrolled bladder contractions. (For example, it is not due to a urine infection or an enlarged prostate gland.)
Overactive bladder syndrome is sometimes called an irritable bladder or detrusor instability. (Detrusor is the medical name for the bladder muscle.)
Symptoms include:
Urgency. This means that you get a sudden urgent desire to pass urine. You are not able to put off going to the toilet.
Frequency. This means going to the toilet often - more than seven times a day. In many cases, it is a lot more than seven times a day.
Nocturia. This means waking to go to the toilet more than once at night.
Urge incontinence occurs in some cases. This is a leaking of urine before you can get to the toilet when you have a feeling of urgency.
How common is overactive bladder syndrome?
In two large studies, it was found that about 1 in 6 adults reported some symptoms of an overactive bladder. Symptoms vary in their severity. About 1 in 3 people with an overactive bladder have episodes of urge incontinence.
What causes overactive bladder syndrome?
The cause is not fully understood. The bladder muscle seems to become overactive and contract (squeeze) when you don't want it to.
Normally, the bladder muscle (detrusor) is relaxed as the bladder gradually fills up. As the bladder is gradually stretched, we get a feeling of wanting to pass urine when the bladder is about half full. Most people can hold on quite easily for some time after this initial feeling until a convenient time to go to the toilet. However, in people with an overactive bladder, the bladder muscle seems to give wrong messages to the brain. The bladder may feel fuller than it actually is. The bladder contracts too early when it is not very full, and not when you want it to. This can make you suddenly need the toilet. In effect, you have much less control over when your bladder contracts to pass urine.
In most cases, the reason why an overactive bladder develops is not known. This is called overactive bladder syndrome. Symptoms may get worse at times of stress. Symptoms may also be made worse by caffeine in tea, coffee, cola, etc, and by alcohol (see below).
In some cases, symptoms of an overactive bladder develop as a complication of a nerve- or brain-related disease such as following a stroke, with Parkinson's disease, with multiple sclerosis or after spinal cord injury. Also, similar symptoms may occur if you have a urine infection or a stone in your bladder. These conditions are not classed as overactive bladder syndrome as they have a known cause.
What are the treatments for overactive bladder syndrome?
· Some general lifestyle measures may help.
· Bladder training is the main treatment. This can work well in up to half of cases.
· Medication may be advised instead of, or in addition to, bladder training.
· Pelvic floor exercises may also be advised in some cases.
Some general lifestyle measures that may help
- Getting to the toilet. Make this as easy as possible. If you have difficulty getting about, consider special adaptations like a handrail or a raised seat in your toilet. Sometimes a commode in the bedroom makes life much easier
- Caffeine. This is in tea, coffee, cola, and is part of some painkiller tablets. Caffeine has a diuretic effect (will make urine form more often). Caffeine may also directly stimulate the bladder to make urgency symptoms worse. It may be worth trying without caffeine for a week or so to see if symptoms improve. If symptoms do improve, you may not want to give up caffeine completely. However, you may wish to limit the times that you have a caffeine-containing drink. Also, you will know to be near to a toilet whenever you have caffeine.
- Alcohol. In some people, alcohol may make symptoms worse. The same advice applies as with caffeine drinks
- Drink normal quantities of fluids. It may seem sensible to cut back on the amount that you drink so the bladder does not fill so quickly. However, this can make symptoms worse as the urine becomes more concentrated, which may irritate the bladder muscle. Aim to drink normal quantities of fluids each day. This is usually about two litres of fluid per day - about 6-8 cups of fluid, and more in hot climates and hot weather.
- Go to the toilet only when you need to. Some people get into the habit of going to the toilet more often than they need. They may go when their bladder only has a small amount of urine so as "not to be caught short". This again may sound sensible, as some people think that symptoms of an overactive bladder will not develop if the bladder does not fill very much and is emptied regularly. However, again, this can make symptoms worse in the long run. If you go to the toilet too often the bladder becomes used to holding less urine. The bladder may then become even more sensitive and overactive at times when it is stretched a little. So, you may find that when you need to hold on a bit longer (for example, if you go out), symptoms are worse than ever.
Bladder training (sometimes called bladder drill)
The aim is to slowly stretch the bladder so that it can hold larger and larger volumes of urine. In time, the bladder muscle should become less overactive and you should become more in control of your bladder. This means that more time can elapse between feeling the desire to pass urine and having to get to a toilet. Leaks of urine are then less likely. A doctor, nurse, or continence advisor will explain how to do bladder training. The advice maybe something like the following:
You will need to keep a diary. On the diary make a note of the times you pass urine and the amount (volume) that you pass each time. Also, make a note of any times that you leak urine (are incontinent). Your doctor or nurse may have some pre-printed diary charts for this purpose to give you. Keep an old measuring jug by the toilet so that you can measure the amount of urine you pass each time you go to the toilet.
When you first start the diary, go to the toilet as usual for 2-3 days at first. This is to get a baseline idea of how often you go to the toilet and how much urine you normally pass each time. If you have an overactive bladder you may be going to the toilet every hour or so, and only passing less than 100-200 ml each time. This will be recorded in the diary.
After the 2-3 days of finding your baseline, the aim is then to hold on for as long as possible before you go to the toilet. This will seem difficult at first. For example, if you normally go to the toilet every hour, it may seem quite a struggle to last one hour and five minutes between toilet trips. When trying to hold-on, try distracting yourself.
For example:
· Sitting straight on a hard seat may help.
· Try counting backwards from 100.
· Try doing some pelvic floor exercises (see below).
With time, it should become easier as the bladder becomes used to holding larger amounts of urine. The idea is gradually to extend the time between toilet trips and to train your bladder to stretch more easily. It may take several weeks, but the aim is to pass urine only 5-6 times in 24 hours (about every 3-4 hours). Also, each time you pass urine you should pass much more than your baseline diary readings. (On average, people without an overactive bladder normally pass 250-350 ml each time they go to the toilet.) After several months you may find that you just get the normal feelings of needing the toilet, which you can easily put off for a reasonable time until it is convenient to go.
Whilst doing bladder training, perhaps fill in the diary for a 24-hour period every week or so. This will record your progress over the months of the training period.
Bladder training can be difficult but becomes easier with time and perseverance. It works best if combined with advice and support from a continence advisor, nurse, or doctor. Make sure you drink a normal amount of fluids when you do bladder training (see above).
Medication
If there is not enough improvement with bladder training alone, medicines in the class of drugs called antimuscarinics (also called anticholinergics) may also help. They include oxybutynin, tolterodine, trospium chloride, propiverine, and solifenacin. These also come in different brand names. They work by blocking certain nerve impulses to the bladder, which relaxes the bladder muscle and so increases the bladder capacity.
Medication improves symptoms in some cases, but not all. The amount of improvement varies from person to person. You may have fewer toilet trips, fewer urine leaks, and less urgency. However, it is uncommon for symptoms to go completely with medication alone. A common plan is to try a course of medication for a month or so. If it is helpful, you may be advised to continue for up to six months or so and then stop the medication to see how symptoms are without the medication. Symptoms may return after you finish a course of medication. However, if you combine a course of medication with bladder training, the long-term outlook may be better and symptoms may be less likely to return when you stop the medication. So, it is best if the medication is used in combination with bladder training.
Side effects are quite common with these medicines but are often minor and tolerable. Read the information sheet, which comes with your medicine for a full list of possible side effects. The most common is a dry mouth, and simply having frequent sips of water may counter this. Other common side effects include dry eyes, constipation and blurred vision. However, the medicines have differences, and you may find that if one medicine causes troublesome side effects, a switch to a different one may suit you better.
Pelvic floor exercises
Many people have a mixture of overactive bladder syndrome and stress incontinence. Pelvic floor exercises are the main treatment for stress incontinence. Briefly, this treatment involves exercises to strengthen the muscles that wrap underneath the bladder, uterus (womb) and rectum. For details, see separate leaflets called 'Stress Incontinence' and 'Pelvic Floor Exercises'.
It is not clear if pelvic floor exercises help if you just have overactive bladder syndrome without stress incontinence. However, pelvic floor exercises may help if you are doing bladder training (see above).
Surgery
If the above treatments are not successful, surgery is sometimes suggested to treat overactive bladder syndrome. Procedures that may be used include:
· Sacral nerve stimulation. An overactive bladder can be treated by sacral nerve stimulation. A small pulse generator device is implanted under the skin of the buttock to send a burst of electrical signals to the nerves that control the bladder.
· Augmentation cystoplasty. In this operation, a small piece of tissue from the intestine is added to the wall of the bladder to increase the size of the bladder. However, not all people can pass urine normally after this operation. You may need to insert a catheter (a small tube) into your bladder in order to empty it.
· Urinary diversion. In this operation, the ureters (the tubes from the kidneys to the bladder) are routed directly to the outside of your body. There are various ways that this may be done. Urine does not flow into the bladder. This procedure is only done if all other options have failed to treat your overactive bladder syndrome.
Treatment with botulinum toxin A
This is an alternative treatment to surgery if other treatments including bladder training and medication have not helped your symptoms. The treatment involves injecting botulinum toxin A into the sides of your bladder. This treatment has an effect of damping down the abnormal contractions of the bladder. However, it may also damp down the normal contractions so that your bladder is not able to empty fully. If you have this procedure you usually need to insert a catheter (a small tube) into your bladder in order to empty it.
Note: botulinum toxin A has now been licensed (approved) for the treatment of overactive bladder syndrome. Make sure that you discuss this procedure fully with your doctor and understand all of its risks and benefits before you go ahead with it.
Continence adviser
Your GP may refer you to the local continence adviser. Continence advisers can give advice on treatments, especially about bladder training and pelvic floor exercises. If incontinence remains a problem, they can also give lots of advice on how to cope. For example, they may be able to supply various appliances and aids to help, such as incontinence pads, etc.
Further help and information contact the Continence Helpline 0800 650 659 or go to www.continence.org.nz
Acknowledgement: Bladder and Bowel Foundation, United Kingdom.